I’m on orientation for two weeks — I get 4 patients in the morning, and 4 in the afternoon. That’s supposed to give me lots of time to get to know my patients, the charting system, and how things work in the organization with patient flow and all.
It’s been a year and a half since I graduated. The only other times I’ve laid hands on “patients” is when I have been doula to the friends and family that asked for pregnancy, birth, and postpartum support. So here I am, getting the hang of using the speculum again, and I’m having to figure out simple things like how to best help a patient sit up on the table after a bout in the stirrups. Other things, like listening to women, talk before touch, and explaining what I’m doing, haven’t changed.
As I am getting oriented to the organization and to my patients, and getting used to being in charge (not a student any more!), I am trying to also orient my patients to their own bodies.
Today, I found Nabothian cysts on two patients. I actually had not seen any on any patients while a student, so both times, they threw me off — sending me to investigate first with my heavy edition of Varney’s Midwifery and then to consult with my collaborating physician (OB).
First, you have to get a good view of the cervix. The cervix is at the “back” of the vagina. In some women, it may be tilted down (toward the back) or tilted up (toward the abdomen). In many people, it can be found “midline,” or straight to the back if you are looking into the vagina head-on. The cervix is the mouth to the uterus — it’s where the sperm has to travel to get into the uterus in order to pass to the fallopian tubes for fertilization to occur. Most of us think about the cervix because of the pap smear, HPV, and cervical cancer. It’s also the opening that will dilate when a pregnant woman is in labor, so the baby can pass through the uterus to the vagina and out into the world.
So…to find the cervix on an exam. We usually do the speculum exam before anything else, so as not to mess anything up first by stirring the pot. This has a disadvantage, however. If you haven’t done a digital (finger) exam first, you don’t necessarily know where to look for the cervix. It could be in any of the three positions I mentioned, and you really can’t tell from looking at a patient where her cervix might be found. You also may not know what size speculum she may need.
“M’am, please place your feet on the stirrups here. Good! Now, keep your feet here, and try to flop your knees out toward the wall. Wiggle your toes to relax your bottom. Great! Now, here is my hand [touches back of left hand to patient’s inner right thigh]. I’m going to place the speculum now. Lots of pressure.”
Placing the speculum at a 30* angle to the floor of the vagina and pressing down ensures you aren’t putting pressure on the bladder or clit. From there…you have to kind of wiggle the speculum toward the back of the vagina, then open slowly while trying to visualize the round shiny part with the little opening. Flat if she’s had babies; small and round if she has not.
Then: what is that? You want it to be round, shiny, and pink. Some might have an area of pink around the os (inner hole) — “ectropian.” Cervicitis, or inflammation of the cervix, can be seen with sexually transmitted infections chlamydia or gonorrhea, and usually comes with discharge escaping from the os.
What I wasn’t expecting today was present for two women I cared for: 1-2 centimeter bumps on the cervix; round to more ovoid, white with pink/reddish edges, and non-tender when touched with the fox swab (giant Q-tip). To give you a visual, here is a “normal” versus a cervix where there are Nabothian cysts:
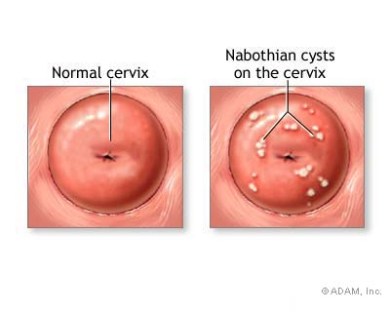
Of course, these are cartoon drawings…but you get the idea. After I took samples from the os for a pap test, STI screen, and a culture of the bump, I did a “bimanual” exam — meaning, I checked her pelvic organs using both hands. Internally, I found her cervix with my right hand. There was a hardened area on her lower cervix, but it was not tender or painful for her as I moved the cervix with one hand internally and then pressed the uterus down with my other hand.
Nabothian cysts usually resolve on their own, and are considered a benign condition. You can read more about them on this delightful website: http://www.beautifulcervix.com/nabothian-cyst/
I had the pleasure of learning alongside my patients today…and now have the pleasure of sharing with you, dear reader. Now: tell your friends! Get to know your cervix. Find out what size speculum works best for finding your cervix, so you can tell future health care providers which size they should reach for when doing your exam.
And…be nice to your cervix! Protect it from possible exposure to HPV by getting the HPV vaccine; by using condoms if you are at risk for STIs; and by following pap guidelines for prevention of cervical cancer. Talk to your partner(s) about it, and ask your health care provider for more information or for help navigating your sexual health and safety.




